
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Aysenur Cetin Uceriz* and Pınar Yel
Corresponding Author: Aysenur Cetin Uceriz, Department of Nursing, Halic University, Istanbul, Turkey.
Received: December 23, 2024 ; Revised: January 03, 2025 ; Accepted: January 06, 2025 ; Available Online: January 08, 2025
Citation: Uceriz AC & Yel P. (2025) Evaluation of a Patient with Heart Failure Using Leininger's Sunrise Model. J Nurs Midwifery Res, 4(1): 1-6.
Copyrights: ©2025 Uceriz AC & Yel P. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
This case report details the nursing care process for a patient diagnosed with heart failure, who faced significant barriers in accessing health services. It examines the health issues arising from economic and communication challenges experienced by an individual working in our country. The report also addresses the patient's cultural characteristics, beliefs, values, and health perceptions, leading to a personalized nursing process that respects individual differences. In the care process, transcultural nursing principles facilitated effective communication with the patient, highlighting the impact of cultural awareness on health care. Approaches were also developed to address both cultural adaptation and the physical needs of the individual, alongside providing training and guidance for the patient and their family. The study concludes that the transcultural nursing approach serves as an effective model for caring for individuals from diverse cultural backgrounds. This model enhances not only the physical health of these individuals but also aids in their cultural adaptation and integration into the health system. The findings underline the critical need for cultural sensitivity and personalized nursing care, demonstrating that this approach elevates the quality of health services by offering innovative perspectives in nursing practices. Thus, it serves as a vital reference for fostering and sharing culturally aware practices within the nursing profession.
Keywords: Heart failure, Immigrants, Nursing care, Sunrise model, Transcultural nursing
INTRODUCTION
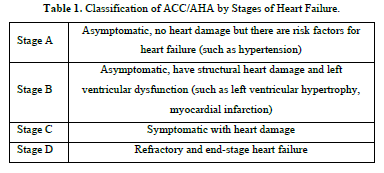
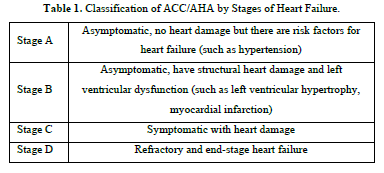
Heart failure (HF) is a clinical condition caused by cardiac structural and functional anomalies, accompanied by typical symptoms such as shortness of breath, fatigue, and edema as a result of low cardiac output and/or high intracranial pressure during rest or exercise. Some findings include increased jugular venous pressure, pulmonary rales, and peripheral edema [1]. The American Heart Association (AHA) estimates that a 46% increase in heart failure is expected from 2012 to 2030. It predicts that by 2030, more than 8 million people in the 18 and over age group in the USA will have heart failure. In our country, the HAPPY study conducted in 2012 (Research on Prevalence and Determinants of Heart Failure in Turkey) determined that there is a patient population of over two million [2,3]. There are many causes in the etiology of heart failure, such as valve diseases, congenital heart diseases, pulmonary diseases, connective tissue diseases, and infections. For its diagnosis, it is necessary to have physical examination findings and objective results of structural or functional disorders, along with typical symptoms. According to the Heart Failure Staging of the American College of Cardiology/American Heart Association (ACC/AHA), heart failure patients are examined in four stages, with the first two stages (A and B) being asymptomatic and at risk for the development of heart failure, while stages C and D include symptomatic heart failure patients (Table 1) [4].
Symptomatic improvement should usually be observed in patients who are initiated with appropriate treatment by determining the stage of heart failure. Even if patients are asymptomatic after diagnosis, appropriate treatment approaches should be followed [1,4]. Advanced-stage heart failure is a period in which patients continue to have complaints and HF findings even during mild exertion and/or rest, despite optimal medical treatment, device therapy or surgical interventions, and many important decisions need to be made in the management of the disease such as recurrent hospitalizations, the need for inotropic treatment, the placement of mechanical support devices or heart transplantation, and survival is significantly shortened for many patients [5]. The European Society of Cardiology (ESC) QM guideline includes multidisciplinary care management programs other than medical treatment. It also includes programs for care organization, lifestyle advice, exercise training, follow-up and observation, palliative and end-of-life care, and combating frailty and cognitive disorders [6,7]. The lifestyle behaviors of individuals vary according to the characteristics of the society in which they live, their religious beliefs, educational status, and culture. Nurses need to consider the cultural characteristics of individuals in patient care. Care is not only a concept associated with illness or health but also a fundamental element of the cultural outlook. In nursing care, culturally weighted situations, such as attitudes about health and illness, family life, sexuality, nutrition, and dressing habits, are important parts of holistic nursing care. It is necessary to consider the individual as a whole in terms of physical, spiritual, social, and mental aspects, and each individual lives differently within their cultural environment. In this sense, the Transcultural Care Theory guides nurses in care practices, which emerged from the need to care for individuals from different cultures [8].
TRANSCULTURAL CARE THEORY (LEININGER'S SUNRISE MODEL)
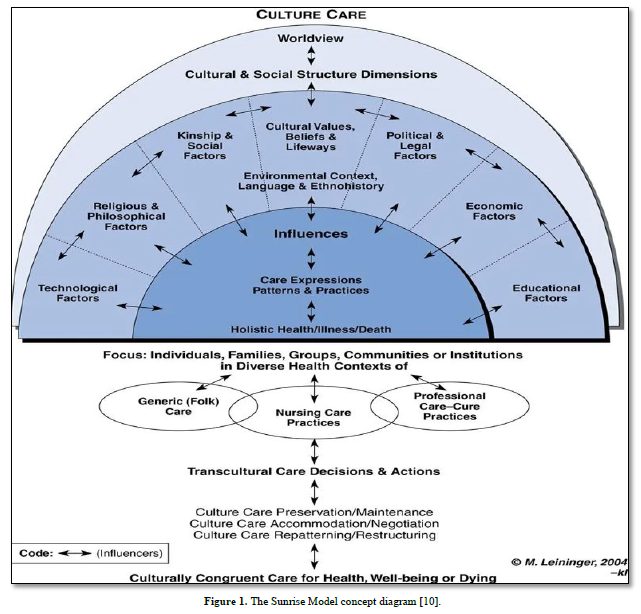
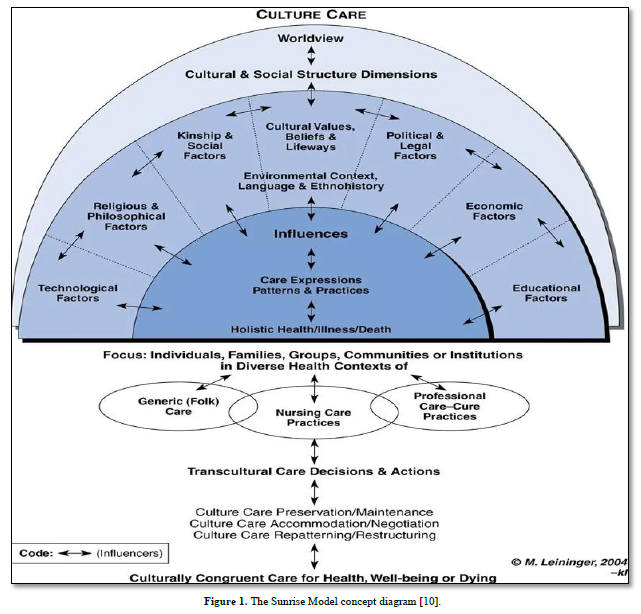
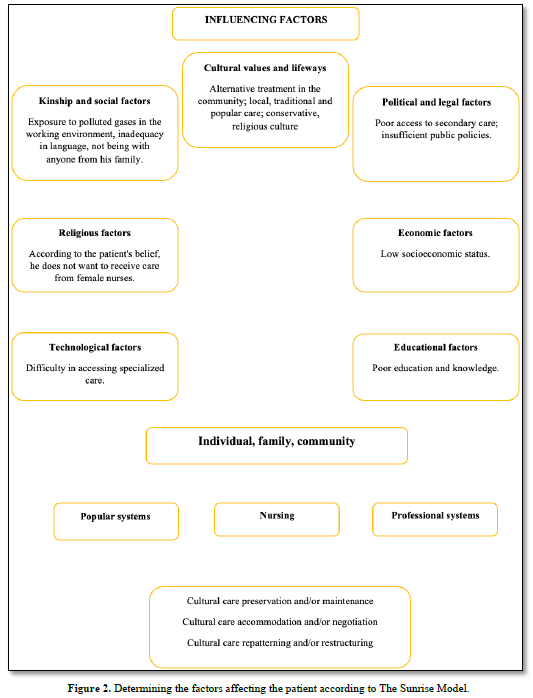
Culture includes the values, beliefs, behaviors, rules, customs and traditions, lifestyle and practices of a particular society that are learned and passed on from generation to generation. According to Madeleine Leininger, the founder of intercultural nursing, culture; It is the accumulation of knowledge about values, beliefs, roles and lifestyles that is learned and passed on to generations [9]. Leininger, the founder of transcultural nursing, defines transcultural nursing as a field of nursing that reveals scientific and humanist knowledge, puts this knowledge into use in the fields of "special-culture" and "universal-culture", focuses on health-disease care, a subculture that respects beliefs and values, and comparative research and analysis of different cultures [10]. Culturally sensitive nursing practices include identifying cultural needs, understanding the cultural connections of families and individuals in order to provide care without affecting the family's cultural belief system, and using emotional strategies to help caregivers and recipients achieve mutual goals. Therapeutic relationship building, appropriate and responsive care, and treatment can begin with a transcultural nursing approach [11]. Nurses with different cultures also care for individuals, families and community groups with different cultural characteristics. Just as nursing care is affected by the cultural characteristics of the individual receiving care, the culture of the nurse also affects the care initiatives she plans [12]. By creating the 'sunrise' model, Leininger talked about the necessity of cultural care in nursing care, created a theoretical method that guides studies on cultural health beliefs, and developed standard principles for nursing. These factors in Leininger's Sunrise Model are listed as the individual's worldview, kinship and social factors, cultural values, beliefs and lifestyles, religious/spiritual/philosophical factors, technological factors, economic factors, political and legal factors, educational factors, language and communication factors, emic and ethical care beliefs and practices, and general and specific nursing care factors [13,14] (Figure 1).
According to Leininger's theory, the initiatives and decisions of nurses who know and respect cultural care values will make a significant difference in the continuation of health and the improvement of diseases. Three main issues that nurses should especially consider are:
CASE REPRESENTATION
In this study; the personal data of N.A., an irregular immigrant who came to Türkiye for work, were collected and nursing practices were discussed according to the Transcultural Care Theory (Leininger's Sunrise Model).
Introductory Features
Mr. N.A.; The 35-year-old married father of four said he left his family in his home country and came to Türkiye about six months ago to work. During the time he lived in Türkiye, he learned to speak very little Turkish. Our detailed communication with the individual is provided by the colleague with whom he came to the hospital. A year ago, he was diagnosed with heart failure in the hospital where he applied due to shortness of breath and stated that he received his treatment in his country without interruption. He explained that he ran out of medicines shortly after coming to Türkiye and did not apply to any health institution due to financial difficulties. The patient, who had a history of hypertension in his background, was brought to the hospital by his colleague with complaints of shortness of breath and chest pain. The patient works as a worker in the plastics factory, and four people stay together in the container houses of the factory where he works. It has been stated that the individual who does not have a history of active smoking smokes intensively in the environment where he stays together. Vital signs taken when the patient arrives at the hospital; Blood pressure: 140/80 mmHg, Pulse: 122 /min, Respiratory Rate: 26/min, Oxygen Saturation: 96. As a result of the physical examination and diagnostic tests, 25% EF was detected and the patient was hospitalized with the diagnosis of congestive heart failure + hypertension. Treatment was started in line with the physician's directive. The individual was admitted to the service and oxygen therapy was started at 3 ml/min at the physician's request. A urinary catheter was inserted in order to follow up what he took and removed. In the evaluation made using the fall risk rating scale, it was determined that the risk score was high (ITAKI score: 12). It has been observed that the individual is anxious due to the shortness of breath he is experiencing. After hospitalization, it has been observed that he has a timid attitude towards the nurse during applications such as vascular access and blood pressure measurement. In the detailed communication established through his colleague next to him, he stated that it was forbidden for the lady other than his wife to touch him due to his religious beliefs.
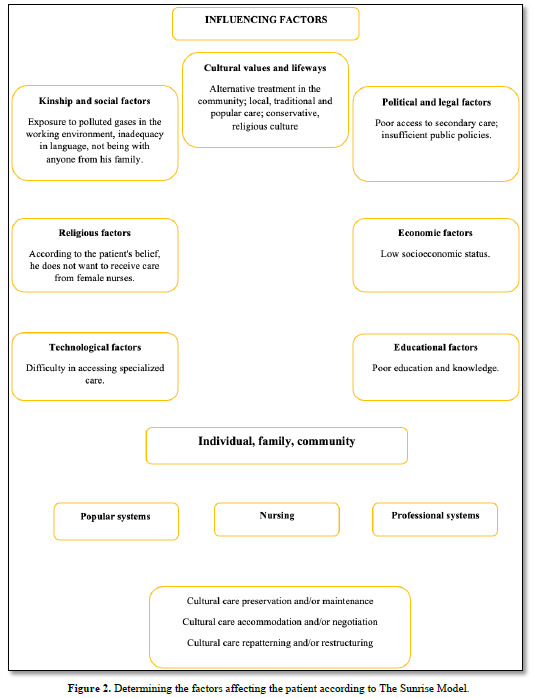
During the provision of health care services, the patient stated that they preferred male health workers, especially in therapeutic intervention procedures, and since the nurses working in the service were women, a male health worker from the other unit was asked to help him wear it after urine. Nurses working on that day for health care practices were informed in terms of paying attention to the sensitivity of the patient in this regard, and the necessary treatment program was implemented by taking care to maintain the patient-nurse distance. It was observed that N.A., who left her family there and came to our country due to economic conditions because she did not have the opportunity to work due to the war in her country, worsened the symptoms of the disease. It has been determined that the treatment of the patient, who did not go to any health institution due to economic reasons and could not take his medicines when his drugs ran out, was disrupted. It was stated that the individual working in the plastics factory went out to get air when he had severe shortness of breath, and after resting for a while, he started working because he had to return to work. He stated that he often went out to breathe because of the smoking in the environment where they stayed together. It was observed that the patient, who stated that his shortness of breath today was severe and he felt faint, had a fear of death. In the light of all this information, the evaluation process of the case within the scope of transcultural care theory (Leininger's Sunrise Model) is presented in Figure 2.
In order to reduce the anxiety of being away from his family and the health problem he is experiencing; the patient is given the opportunity to make a phone call when he feels better. For the patient, who did not indicate that he was in a hospital environment because he did not want to worry his children and wife, it was possible to conduct an interview under appropriate environmental conditions. It has been learned that the patient, who is fed with the foods offered to them by the workplace, generally eats carbohydrate-based and does not pay attention to salt and water restriction. The individual, who stated that he used salt a lot due to the tastelessness of the food, was trained by using visual shapes that he should restrict salt due to his diseases. They were informed about the importance of using their medications regularly.
CONCLUSION
Transcultural nursing is gaining more and more importance in the health care processes of individuals who have had to leave their countries due to wars, economic difficulties and other socio-political reasons, especially in recent years. Nurses should conduct a brief cultural assessment when they first contact individuals and elaborate on this assessment in line with the individual's needs [17]. Research conducted in Türkiye reveals that immigrants who come to the country for work purposes are generally only primary school graduates or only know how to read and write. It has been established that these individuals provide their livelihood largely with the help of the municipality or the public. It has been stated that most of the immigrants do not have access to health services due to financial inadequacies and language barriers, which leads to the prevalence of chronic diseases [18,19]. Within the scope of this study, an individual who came to Türkiye six months ago to work, but could not benefit from health services due to financial inadequacies and language barriers, was considered. Necessary nursing care was provided to the individual by respecting their cultural values and norms. Individual nursing care provided with cultural sensitivity has strengthened the communication between the patient and the healthcare worker, enabling the individual to participate more actively in the care process. In addition, by reducing the barriers to an individual's access to healthcare, it has increased the effectiveness of disease management and contributed to the improvement of the overall quality of life. Such an approach not only contributes to the physical well-being of the individual, but also supports mental and social well-being, allowing for a more comprehensive level of health to be achieved. In this context, nurses should adopt a holistic approach in health care practices; It is of great importance that individuals do not ignore the lifestyle, cultural norms and health behaviors of the society they live in.
No Files Found




Internationally Accepted
Share Your Publication :